The Science
Waist circumference predicts lifespan. Hunger is a mineral deficit, not a need for GLP-1s. The cutting-edge science that maximizes your longevity — and makes you unstoppable.

01 · Fasting, Belly Fat & Longevity
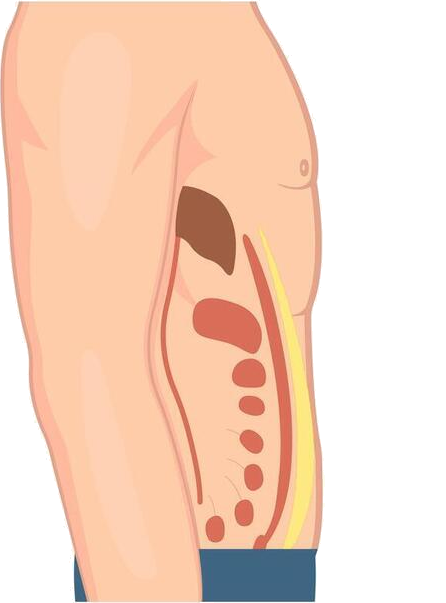
The fat around your middle is the fat that matters.
Visceral fat — the fat packed around your organs, hidden beneath the outer subcutaneous layer — is one of the strongest predictors of premature death, more telling than weight or BMI alone. The good news: it responds to when you eat, not just what.
An 8-hour eating window cuts visceral fat — as sustainably as cutting calories.
Time-restricted eating reduced visceral fat comparably to daily calorie restriction in a randomized trial. The fasting hours also trigger autophagy, the cell's natural cleanup.
He et al., Cell Reports Medicine, 2022. →Waist size tracks with how long you live.
In large cohorts, a larger waist circumference predicted higher all-cause mortality independent of BMI.
Cerhan et al., Mayo Clinic Proceedings, 2014. →Sugar feeds visceral fat; salt does not.
Fructose-sweetened drinks increased visceral fat and worsened insulin sensitivity in a controlled trial — which is why Zero Hunger Water is sugar-free by design. Remove the sugar, keep the salt.
Stanhope et al., J Clin Invest, 2009. → Bonus · Watch
Bonus · WatchThe day Dr. Oz measured my belly.
2008, Columbia University. The on-air moment Dr. Oz measured Jorge's waist — and made visceral belly fat impossible to ignore.
Watch the moment →02 · The Mineral–Hunger Connection
Much of what you call hunger is a mineral signal.
Modern diets and fasting both deplete sodium, potassium, and magnesium. When those minerals run low, the body doesn't ask for them directly — it ramps up the drive to eat. Replace what's missing, and a large share of that "hunger" quiets at its source.
Low sodium drives salt- and food-seeking.
When sodium is depleted, the brain's drive toward salt and palatable food rises sharply — a well-mapped physiology, not a theory.
Morris, Na & Johnson, Physiology & Behavior, 2008. →Magnesium steadies blood sugar — and steadier blood sugar means fewer cravings.
In randomized trials, oral magnesium improved insulin sensitivity and fasting glucose. About half of U.S. adults fall short of the magnesium target.
Meta-analysis of RCTs, 2016. →Electrolytes make fasting livable.
Replacing sodium, potassium, and magnesium relieves the fatigue, headache, and hunger that derail a fast — which is why most members sip minerals across their fasting window rather than reaching for food.
Electrolyte balance during fasting — review. →03 · GLP-1s Adapt & Fade
GLP-1 works — until the body adapts.
Every powerful weight-loss tool runs into the same wall: the body fights back. GLP-1 medications produce strong appetite suppression at first, but the effect plateaus around 60–72 weeks — and when the medication stops, most of the lost weight returns, roughly two-thirds within a year. Restoring minerals is different: there is no known tolerance or adaptation to them. As long as the deficiency is corrected, the effect holds.
GLP-1 appetite suppression plateaus — tachyphylaxis.
GLP-1 medications produce strong appetite suppression at first, but the effect plateaus around 60–72 weeks as the body adapts. This is metabolic adaptation, and it applies to nearly every powerful weight-loss tool.
Wilding et al. (STEP-1), semaglutide, NEJM 2021; Jastreboff et al. (SURMOUNT-1), tirzepatide, NEJM 2022. →Most lost weight returns after the medication stops.
When the drug is withdrawn, roughly two-thirds of the lost weight returns within a year. Continued dosing maintains it; stopping reverses it.
Wilding et al. (STEP-1 extension), Diabetes Obes Metab 2022; (SURMOUNT-4), JAMA 2024. →Minerals don't fade — there is no tolerance to them.
Unlike drugs the body adapts to, minerals are nutrients the body needs daily. There is no known tolerance or adaptation to them — as long as the deficiency is corrected, the effect holds.
Hall KD. Metabolic adaptations to weight loss across diet, drug, and surgery. Obesity, 2024. →Important. Zero Hunger Water does not contain GLP-1 and is not a GLP-1 drug or a substitute for one. Always talk to your doctor before starting, changing, or stopping any medication.
04 · The Studies — Reference Materials
References
- 01.Morris MJ, Na ES, Johnson AK. Salt craving: the psychobiology of pathogenic sodium intake. Physiology & Behavior. 2008. PMID 18514747.
- 02.Meta-analysis of randomized controlled trials: oral magnesium supplementation, insulin sensitivity and fasting glucose. 2016. PMID 27530471.
- 03.He M, et al. Time-restricted eating with or without low-carbohydrate diet reduces visceral fat and improves metabolic syndrome: a randomized trial. Cell Reports Medicine. 2022. PMID 36220069.
- 04.Cerhan JR, et al. Waist circumference and all-cause mortality. Mayo Clinic Proceedings. 2014. PMID 24582192.
- 05.Katzmarzyk PT, et al. Waist circumference and mortality risk. Archives of Internal Medicine. 2009.
- 06.Stanhope KL, et al. Fructose-sweetened beverages, visceral adiposity and insulin sensitivity. Journal of Clinical Investigation. 2009. PMID 19381015.
- 07.Wilding JPH, et al. (STEP-1) Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021.
- 08.Jastreboff AM, et al. (SURMOUNT-1) Tirzepatide once weekly for obesity. New England Journal of Medicine. 2022.
- 09.Wilding JPH, et al. (STEP-1 extension) Weight regain after withdrawal of semaglutide. Diabetes, Obesity & Metabolism. 2022. PMID 35441470.
- 10.(SURMOUNT-4) Continued versus withdrawn tirzepatide and weight maintenance. JAMA. 2024.
- 11.Hall KD. Metabolic adaptations to weight loss across diet, drug, and surgery. Obesity. 2024.
Most hunger isn't hunger. It's a mineral deficiency.
Take the 3-minute longevity quizIllustrative — not a claim of specific results. All graphics on this page (visceral-fat animation and adaptation chart) are educational illustrations, not depictions of a specific individual's outcome. These statements have not been evaluated by the Food and Drug Administration. Zero Hunger Water is not intended to diagnose, treat, cure, or prevent any disease, and is not a substitute for medical care or prescribed medication. If you have kidney disease, high blood pressure, heart failure, or take medications that affect potassium (ACE inhibitors, ARBs, or potassium-sparing diuretics), talk with your doctor before increasing your mineral intake.